A year ago, we paid tribute to Jerome Robert Lohez, who perished in the flames and destruction of the World Trade Center.
In his memory, and those of his fellow Americans who died on that horrible day, I'm honored (if saddened) to reprise that post:
As regular InsureBlog readers know, my better half has long maintained that “there are no coincidences.” That is, she believes that everything happens for a reason, although we may not be aware just what that reason is.
As for me, I’ve gradually become 90% convinced that she’s right on this (in everything else, of course, she’s 100% right). But one evening, a few weeks ago, that all changed.
I have a confession: My name is Henry, and I’m a news junkie. It is my habit to stay up way too late reading news blogs. Which I was doing several weeks ago, when I came across an item about one man’s extraordinary effort [ed: back online] to harness the power of the blogosphere, in tribute to our fellow Americans who died in The Towers, exactly five years ago today. The concept was deceptively simple: 2996 victims, 2996 blogs, each one remembering a single person. Bloggers were invited to sign up, and each was assigned – at random – one name.
Stop for a moment, and consider this: one blogger, reading one news item, decides it’s the right thing to do, signs up, and is assigned the name of a person he’s never even heard of, let alone met. We’ll come back to this shortly.
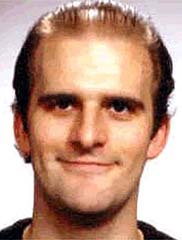
And so I was assigned the name of Jerome Robert Lohez, given a photo of him, and told the briefest of biographical information: age 30, lived in Jersey City, New Jersey.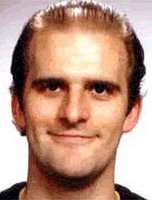 That was it. A name, a face, a place.
That was it. A name, a face, a place. The assignment was simple: On September 11, post his name and picture.
But I’m a news junkie, and that wasn’t good enough. I had to know more about Jerome. So I Googled his name (hey, why not?) and came across a site that CNN put together in December of ’01. It had pictures and names, of course, but I also learned that Jerome, born in France, married Dening Wu some three years before The Towers fell. One month before The Towers fell, Jerome got his Green Card, and the happy couple flew to Europe to celebrate with his family. When they got back, two days before The Towers fell, Jerome told Dening “Only in New York do we have so much sunshine." That was Sunday, September 9, 2001.
On Tuesday morning, he left for work. And The Towers fell.
And now we've come full circle: One. Random. Name.
Jerome didn’t just work in The Towers. He worked for Empire Blue Cross and Blue Shield. He worked in the insurance industry.
90% doesn’t cut it anymore.
Thank you, Jerome, for the lives you touched, the joy you brought, your love for New York and America, and for the privilege of paying you tribute.
Au revoir, Monsieur Lohez, au revoir.








{kind=link}
{kind=link}
{kind=link}
{kind=link}